
Luca Martinelli
Basic
aspects regarding the classification of articulators
Publication
no. 25 - 27 June 2013
1.
Articulators
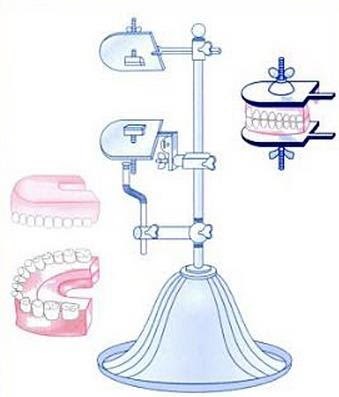
Articulators are mechanical
devices that simulate the skeletal system, or rather simulate the movement of
the temporomandibular joint (Fig. 1).
{kind=link}

Fig.
1
Each
part of an articulator has a more or less conventional name. The terms utilized
are shown in Fig. 2, which depicts an average value articulator, as this is the
type most commonly used in laboratories.
{kind=link}

Fig. 2
*Notes:
See
publication no.
6 – Basic aspect regarding articulators
2. Historical notes
The
origins of the articulator date back to somewhere between 1750 and 1805. In
1756, in fact, German dentist Phillip Pfaff (Fig. 3) took the first wax
impressions and cast the first models, which were indispensable for the
articulator's existence. He is also credited with having invented the wax bite,
although this cannot be unequivocally confirmed. The date is given by the
publication of work entitled Abhandlung von den Zaehnen des menschlinen Koerpes und
deren Krankeiten, which was
published precisely in that year (Fig. 4).

{kind=link}
Fig. 3
Fig. 4
In 1805, master dental surgeon
Jean Baptiste Gariot created the Plaster articulator (the Ante-Litteram
articulator), also known as the "Oiled Board" (Fig. 5), which was
basically an extension of the models with two semi-circular reference points
made upon one of them using the fingers (it was therefore also known as the
finger articulator).
The
date is given by references to the device in Gariot's essay entitled Traité des
maladies de la bouche (Fig.6)
{kind=link}

Fig.
5
Fig.
6
A
number of different variations of this articulator were developed over time (in
the meantime it also came to be known as the Slab Articulator - Fig. 7) and it
remained in use up until the twentieth century. In fact, it was even described
by several authors, such as Richarson in 1860 Coles in 1876, Peezo in 1926,
Essing in 1937, etc.
{kind=link}

Fig.
7
Although
a number of non-patented articulators were also successful, over 40 patents
were filed in America between 1860 and 1910, and in the meantime the Barn Door
Hinge Articulator was developed (Fig. 8), or rather an articulator made using
the hinge of a barn door (hence the name).
{kind=link}

Fig.
8
Meanwhile the articulators
began to take on their first names, like Antagonizing frames, Occluding frames,
Occlusion frames and Antagonizers.
In 1840, James Cameron became
the first person to patent an articulator (Fig. 9).
{kind=link}

Fig.
9
In 1850, Tomas W. Evanz filed
the second patent for an articulator, which at the time was perhaps the best
known throughout the world: the occluder (Fig. 10).
{kind=link}

Fig.
10
The
field of articulators soon exploded and was populated by numerous models, some
of which were quite fanciful. Many of these can be viewed on the website for
the UTHEALTH School of Dentistry - University of Texas,
which indicates the dates of the patents or the ideas and the names of their
inventors, and shows the articulators themselves from various angles, including
detailed views.
A brief photographic overview of a
number of articulators from the past
{kind=link}

{kind=link}

{kind=link}

{kind=link}

3. Articulator classification
Articulators
are divided into categories and classes in order to distinguish their main
features and operating principles.
3.1 Arcon and non-Arcon
Categories (The acronym ARCON stands for:
ARticulator CONdyle (a term coined by Bengstrom in 1950)
The
first subdivision is into two categories, and is based on the type of hinge
axis joint.
This
joint can be shaped and positioned differently depending on the type of
articulator and the manufacturer.
Based
on this, the articulators are divided into two large families:
ARCON
and NON-ARCON.
3.2 ARCON Articulators
ARCON
type Articulators have the condyle on the uprights of the articulator's frame
(1-Fig.11) with the glenoid fossa, known as the condylar box, on the upper frame
(2-Fig. 11).
{kind=link}

Fig.
11
The two parts can be separated.
3.3
NON-ARCON Articulators
NON-ARCON
Articulators , on the other hand, have the condyle on the upper frames,
practically an extension of its hinge axis (1-Fig. 12), while the condylar box
is located on the frame's uprights (2-Fig. 12).
{kind=link}

Fig.
12
The
two parts generally cannot be separated, even though a number of non-Arcon
average value articulators with separable frames can now be found on the
market.
4. Classes and sub-classes
These
articulators in turn are divided into classes and subclasses.
There
are at least a dozen different classifications, based on the type of
articulator, the occlusal theory or the type of registrations, etc. The most
common classification is that according to Heartwell.
4.1 Classification based on the
functions
Class I. A simple holding instrument capable of
accepting a single static registration. Vertical motion is possible.
Class II. An instrument that permits horizontal as well
as vertical motion but does not orient the motion to the temporomandibular
joints.
Class III. An instrument that simulates condylar
pathways by using averages or mechanical equivalents for all or part of the
motion. These instruments allow for orientation of the cast relative to the
joints and may be arcon or nonarcon instruments. (Arcon articulator - An
articulator that maintains anatomic guidelines by the use of condylar analogs
in the mandibular element and fossa assemblies in the maxillary element.)
Class IV.
An instrument that will accept three dimensional dynamic registrations. These
instruments allow for orientation of the cast to the temporomandibular joints
and replication of all mandibular movements.
These can be summarized as
follows:
Class
I: occluders;
Class II: average value articulators;
Class III: Average value articulators adaptable to semi-adjustable (semi-individual) values;
IV Classe: Individual value articulators.
Class II: average value articulators;
Class III: Average value articulators adaptable to semi-adjustable (semi-individual) values;
IV Classe: Individual value articulators.
4.2
Classification based on the occlusal theories
For example:
1. Bonwill, 1858, Triangular
theory of occlusion
2. Balkwill, 1866, Translating jaw
moved medially
3. Von Spee, 1890, Occlusal plane of
teeth follow a curve
|
4. Snow, 1899, Facebow
5. Christensen, 1901, Opening
of posterior teeth in protrusion
6. Bennett, 1908, Immediate
side shift
7. Gysi, 1910, Demonstrated use
of incisal guide pin. One of the first to allow for side shift
8. Monson, 1916, Spherical
theory of occlusion
9. Hall, 1918, Conical theory
10.Hanau, 1921, Rocking chair
denture occlusion
11.Stanbury, 1929, Positional
records Tripod
12.Meyer, 30's, Chew in
technique
13.Avery Brothers, 1930,
Anti-Monson Reverse curve of Wilson
14.Pleasure, 1930, Anti-Monson
except 2nd molars in balance
15.PMS, 20's, Eliminate
balance, Incisal guidance important, Long centric
16.Gnathology, 20's,
Pantograph, need to reproduce mandibular movements
17.Page, 1950, Transographics.
Page is dead and so is Transographics
18.Gelb, 1970, Cranial
Orthopedics. The condyles assume a certain shape based on mandibular movements
4.3
Classification based on the types of registrations used for programming the
articulator
1.
Inter
Occlusal Record Adjustment
2.
Graphic
record adjustment
3.
Hinge Axis
location for adjusting articulator
4.
Etc.
4.4
Other classifications, including:
Gillis (1926), Boucher (1934)
and Kingery (1934)
Beck’s (1962)
Posselt’s (1968)
Thomas (1973)
Riliani (1980)
Weinberg (1963)
Sharry (1974)
5.
The classification according to Heartwell
As
previously mentioned, this is the most commonly used classification. Let's take
a look at its classes and sub-classes (Fig. 13).
{kind=link}

Fig.
13
Class
I
Individual
value articulators (Fig.14)
These
are also known as four dimensional articulators, as they also record the Bennet
movement's time factor.
Characteristics:
>
Fully adjustable to individual values.
>
They allow for the mandibular movements to be reproduced on the three spatial
planes, which are recorded in their entirety using the pantograph.
>
they respect the Bennet movement in terms of both direction of movement and
chronological sequence (four-dimensional articulators).
>
They are mainly used for complete occlusal rehabilitation and for diagnostics.
They are not widely accepted as of yet due to the high cost of the articulator
and the tools required at the clinic for recording the patient's information,
which are indispensable for programming the articulator itself. Furthermore,
their use also requires considerable experience on the operator's behalf.
>
They allow for the adjustment of:
- 1)
the intercondylar distance;
- 2)
the angle of eminence;
- 3)
the curvature of the path taken by the condyles;
- 4)
the direction of the Bennet movement, or rather the direction assumed by the
rotating condyle during laterality;
- 5)
the time relative to the Bennet movement: the immediate lateral displacement is
expressed in millimetres, the progressive lateral displacement is expressed in
degrees with respect to the sagittal plane, which crosses the point at which
the Bennet progressive begins.
The
front portion of the articulator represents the incisive guide, and it
requires the following adjustments:
1)
the vertical dimension;
2)
the overbite and overjet, expressed in millimetres;
Individual
value articulators require both a kinematic face bow and a pantograph in
order to be programmed.
{kind=link}

Fig.
14
Class 2 Articulators
Sub-class 1
Occluders (Fig.
15)
Characteristics:
>
They only perform the rotation movement of the hinge axis (occlusion);
>
The models are positioned without reference to the planes;
>
They do not allow for the transfer of the vertical dimension (they don't have
an incisive pin);
>
They should only be used for checks in relation to things like intercuspation,
for example, and regardless should not be used for for constructing
made-to-measure medical devices.
>
There are also certain types of occluders (like that shown in the photo) that
have a screw for adjusting the vertical dimension.
{kind=link}

Fig.
15
Average
value articulators (Fig.
16)
Characteristics:
>
These have condylar paths with angles obtained from the statistical average of
the values measured on a significant sample of subjects.
>
They simulate the movements of the T.M.J. with fixed angles of eminence, which
can vary by more or less 30° to 40° depending on the manufacturer.
>
They are equipped with incisive pins for adjusting the vertical dimension;
>
They are used for constructing made-to-measure medical devices;
>
Some models can accommodate registrations made with the face bow for the
transfer of the upper model.
{kind=link}

Fig.
16
Class
2 Articulators
Sub-class
2
Special articulators (Fig.
17)
Characteristics:
These
articulators are also known as "arbitrary" articulators, and are
designed for specific occlusion theories or technical specifications.
Some
are based on Monson's "sphere theory" (which states that all extensions of the teeth's axes have points of
origin located at the level of the ethmoid bone).
Having
previously been abandoned, the spherical cap according to Monson's spherical
theory has been revived in recent years, particularly thanks to Bernard
Jankelson's "Neuromuscular" theory, and is supported, for example, by
Piero Silvestrini, who uses it in articulators locked in the hinge axis
position of movement alone.
This
is the case of the "Terminus", for example, which has been
specifically designed for making prostheses according to Bernard Jankelson's
"Neuromuscular Theory".
{kind=link}

Fig.
17
Class 2 Articulators
Sub-class 3
Sub-class 3
Semi-individual value
articulators (Fig. 18)
Characteristics:
Also
referred to as three-dimensional (semi-adjustable) articulators
> They
have condylar paths that can be adapted to the anatomical features of the
patient;
>
They allow for the patient's angle of eminence to be taken into account;
>
A kinematic face bow is required to transfer the models, although arbitrary
face bows and wax joints are also used.
{kind=link}

Fig.
18
Class 2 Articulators
Sub-class 4
Articulators specifically designed for
removable prostheses alone (Fig.
19)
Characteristics:
>
A number of these have been produced in order to create made-to-measure medical
devices according to specific theories.
{kind=link}

Fig.
19
___________________________________________________________________
Attention:
some of these photos are photos posted on the web, anyone who believes they have the right to object to the use he gives notice, the photos will be removed immediately.
Nessun commento:
Posta un commento
Nota. Solo i membri di questo blog possono postare un commento.