Daniele
Tonlorenzi - Luca Martinelli
Mandibular
stretching
Publication no.
12 - 09 November 2012
1. STRETCHING
1.1 Muscle stretching
Stretching is a method of muscle lengthening already widely
known in traditional medicine. It is used largely in the post-operative
rehabilitation and most people knows it for its applications in sports; muscle
stretching, in fact, allows you to make movements more easily, with a greater
amplitude, while, of course, prevent tearing.
Up to now the most used two kinds of
stretching are: the static stretching, where it is hold a fixed position
keeping the muscle stretched for a few seconds, and the dynamic stretching,
where opening and closing movements of the articulation are repeatedly made in an
effort to propel the muscle into the maximum possible extension range, then
returning to the rest position.
1.2 Dental
stretching (mandibular stretching)
In dentistry muscle stretching is named "Mandibular
stretching". The mandible is in fact involved in a static or dynamic
stretching exercise, but it would be better to say that the elevator muscles
(masseter and temporal) are those involved to allow the opening-closing
movement of the mouth.
In this specialized discipline,
stretching is used for a long time indeed, while remaining mostly unknown to
the vast majority of operators and patients.
The stretching can be done even without
aids, but experience has taught us that you cannot get the hoped benefit, and
in a short time, because it is not a practice easy to control and to be understood
by the patient. Figure 1 shows the representation of a static
stretching exercise done by the patient.
Fig. 1
2. MEDICAL DEVICES FOR MANDIBULAR STRETCHING
To achieve the wanted effect many
devices have been invented over the years to perform assisted stretching, which
is a kind of device that helps the patient to the proper execution of
stretching. They can be summarized in three main types:
2.1. Bite
Perhaps the most known device in
absolute, a sort of “bite” (built with a precise height in order to obtain the
muscle elongation) to be kept in mouth during the day or more easily during the
night for the execution of the static stretching. Generally made of resin, it
is a device specially made for each patient; Fig 2 shows a kind of bite.
Fig. 2
2.2 Distracting splint
Surely less known, it is very similar to
the "orthodontic device for children". This one is used to run the
dynamic mandibular stretching.
It is made of resin and is provided with
springs that allow the opening and closing of the mouth: it permits to perform
a dynamic mandibular stretching.
Even in this case we refer to devices made only and exclusively
for a patient; Figure 3 shows some examples.
The
selection shows the splints by
Rampello-Di
Paola-Roncallo and Rocabado
|
Fig. 3
2.3 Industrial device
The last but not the least, we have a
manufactured device, which allows performing mandibular stretching exercises
indistinctly to any patient.
Originally born for post-operative
rehabilitations, it is used nowadays to exploit at most all the benefits coming
from mandibular stretching.
With these devices you can perform both
dynamic and static stretching even if, being able to choose, it is definitely
more advantageous to perform the dynamic exercise.
There are several types of mandibular
stretching. The best known, protected by patents, are the "THERABITE"
by Swedish company ATOS MEDICAL AB (Fig. 4) and the "SPRING DEVICE"
by Italian QUASAR DENTAL EQUIPMENT (Fig. 5).
Fig. 4 - "Therabite" Fig. 5 - "Spring Device"
3. THE MANDIBULAR STRETCHING EFFECTS
A considerable amount of literature have
been written on the effects of stretching in general, and of mandibular
stretching in particular. Anyone can very easily access plenty of information
on the internet: authors and different works done, from the most unknown to the
most authoritative, from Bachelor's thesis, to monographs, up to texts.
At the end of this short informative
text we will report, as an example but not limited to, a part of bibliographic
references that are available on stretching.
It is important to underline that if you
want to consult the bibliography, you must search the one about the stretching
and not the one about the devices that allow its execution; benefits derive
from the mandibular stretching exercise. The devices are only a mean to run it
in an assisted way, that is to facilitate the execution to both the doctor and patient.
We remind that systems such as bites or
distraction splints are customized medical devices on which a wide literature
about construction criteria and use is available.
The industrial devices, such as the
Therabite and the Spring Device, are CE marked and registered to the Ministry
of the Country of their origin. For these, more than a literature search, it could
be useful a functional or economic evaluation on which one is the easiest to
use or which one, for example, has got a lower cost of purchasing and
maintenance and therefore which is the most accessible to the dentist and/or the patient.
We could briefly summarize the effects
that can be achieved with the stretching in a list that we will show here after,
referring to the use of industrialized devices, because they are those we could
consider the most flexible and the best suitable for random or repetitive
cycles of mandibular stretching.
1 - Trismus and/or mandibular hypomobility treatment;
2 - Pain and temporomandibular disorders treatment in patients
undergoing orthodontic treatment, on which you can not use bite for the presence
of dental attachments;
3 - Pain and inflammation of muscles and of the
temporomandibular joint, prevention of cartilage degeneration treatment;
4 - Muscular relaxation therapy to facilitate the registration
of the intermaxillary relations, to promote the prosthetic treatment, bite
etc..;
5 - Pre-extraction preventive treatment (dental avulsion);
6 - Therapy treatment after maxillofacial surgery;
7 - Care and treatment of bruxism;
8 - Physiological reduction of stress.
3.1 Some examples of how to use mass
production muscle stretching devices
It can’t be ignored that we can’t be "impartial" in
discussing the devices mass producted and in fact we will present the use
opportunities of the Spring Device, however, for intellectual honesty, we must
again point out that attention should focus on mandibular stretching and on the
benefical effects that this has on the patient and not on the device that
allows the assisted exercise; beyond all technical, functional and economic
features, all devices with the same intended use may in fact be suited.
But let's see the method of use:
At first it is recommended to use the device for a few minutes
(e.g. two minutes) gradually increasing the time of use.
Therapy, exercise, must be interrupted in case of pain on the patient.
The exercises then can be resumed gradually after a short period of time
established by the dentist.
3.2 In study
All those who live the experience of dental care with particular
physiological stress can obtain a physiological reduction of this, in practice
it has the same type of effect given by the stress ball to be squeezed in hand,
but much more efficient, which will make the patient more tractable allowing
him at the same time a greater ability to keep the mouth open.
This allows a state of well-being, of mental and physical
balance, a state that, in dentistry, must always be the centre of attention.
If then the dentist is late for the patient's appointment, prior
use of the device allows him to still start the session at the appointed time,
with the next patient.
So the dentist earns those 10/20 minutes that allows him to
reduce the delay and to avoid giving the impression of neglecting the patient
in favour of another one.
3.3 Use of the device at home for
a short period (7-10 days)
In this case it is recommended a cycle of stretching exercises
for at least three times a day, the duration of ten minutes each, for a week
prior to surgery, when it is necessary that the mouth:
- gets greater muscle elasticity, facilitating
prolonged dental sessions. Guided implantology, complex or multiple dental
extractions;
- increases its opening with advantage for the
patient (who suffers less) and for the dentist (that works in a better way);
- increases the opening capacity to make easier and correct the detection
of vertical dimensions and especially where there is the need to recover a
space that in the patient has decreased over time;
- sllows more easily to the neuromuscular system to
"accept" a new vertical dimension (new prosthesis) or changes to the
interdental spacing (e.g. bite).
3.4 Use of the device at home for
a long period also in association with a bite
Always be carried out at least three times a day for 10 minutes.
The guidelines are:
- The presence of pain in the temporomandibular joint.
We recall that the guidelines of the American Academy of
Orofacial Pain recommend, as already mentioned, a multidisciplinary approach to
temporomandibular disorder (TMD).
The recommendation of the Academy is to combine the bite to
physiotherapy; the "spring device" increases the compliance.
This combination is of particular importance in the presence of
bruxism.
- Prolonged use in preventive orthodontics,
especially for adults, particularly whenever a certain muscle contracture
occurs. The onset of pain complicates the case, due to the impossibility of
using a bite in the presence of orthodontic attachments.
- Trismus or hypomobility post Maxillofacial therapy, a patient
suffering from these disorders shall be subjected to guided therapy, perhaps
with periodic check-ups, to relax the muscles and increase joint mobility.
In the case of prolonged treatment over time (several months) it
may be considered the possibility of reducing the frequency of the exercises.
To all this we add that this activity also plays a preventive
role in the degeneration of the TMJ's cartilage.
But all this can perhaps be summarized into a table (Fig. 6)
that as the directions shown so far is always to be considered by way of an
example.
Fig. 6
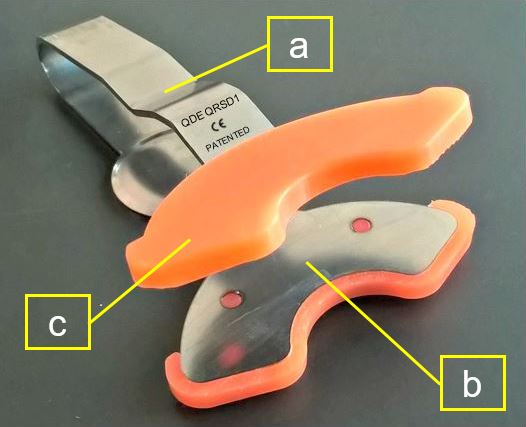
4. SPRING DEVICE - INSTRUCTIONS FOR USE
4.1 Spring Device
The spring device is made of stainless steel (a-Fig. 7) at its ends there are two half-moon-shaped base
plates (c - Fig 7) on which are located two bases made of silicon (d - Fig 7)
upon which the teeth rest.
The silicon base are can be disinfected and sterilized (autoclavable) and so reusable.
Fig.7
4.2 Instructions for use
Take the bases (1-fig. 8) and apply the base on
the device "half-moons" (2 - Fig 8).
Fig. 8
Insert the device in the mouth (Fig. 9) and begin the exercise
involving closing-opening-closing of the jaw.
Fig. 9
5. CONTRAINDICATIONS
Mandibular stretching and especially the use of mass production
devices is contraindicated in cases of:
5.1 Patients with bone disease of the jaw or mandible
e.g.:
1 - Fracture, even suspected of the jaw or mandible;
2- Infections, e.g. osteomyelitis;
3 - Damage caused by osteoradionecrosis.
5.2 Patients with dental
problems:
Before using the device it is important to exclude the presence
of dental problems such as:
1 - Anterior teeth broken, since the closure of the mouth on the
device may cause or facilitate the final rupture, it is true that the force
applied to the "bites" of the device is almost certainly greater than
that exerted during normal chewing hard foods (e.g. bread or meat), anyway it
is good to be cautious;
2 - Presence of fixed prostheses cemented with a temporary
cement to prevent its detachment;
3 - Presence of teeth with large
restorations (perhaps already damaged) as they could get broken.
5.3 Presence of periodontal
disease:
In the case of mobile teeth there is a risk that they may fall.
It is a good practice then assess the stability of any ceramics
fixed prosthesis.
6.CONCLUSIONS
Static mandibular stretching and even more the dynamic one take
advantages to both the patient and the dentist.
The improved mandibular mobility, muscle deprogramming, the
joint movement, are all results that give proved benefits to the patient in
terms of pain relief, improved mood and improved dental treatments.
Even the dentist benefits from mandibular stretching carried out
on the patient, as it is an aid during everyday practices, with a patient more
treatable, and in all the therapies in which it can relieve pain, get more
space and allow for a possible correction of the therapy in place.
The use of medical devices in series for mandibular stretching
facilitates the application of the exercises for all patients, without
distinction, these devices can be used both by dentist and patient with extreme
flexibility in use, time and place of execution.
7 BLIOGRAPHY (annotated)
As mentioned by way of example, but not limited to, we list a
few authors who have dealt with stretching.
Collana di Odontoiatria Pratica
Progressi in odontoiatria vol. 3 Mario Molina Domenico Viscuso Gnatologia Stato
dell’arte sui disturbi cranio-mandibolari UTET. Mandibular stretching in this
book is discussed in detail, but there are no references to the international
literature. Here are a few extracts.
The treatment of myofascial pain
from trigger points, as well as in the identification and elimination of the
causes, consists in stretching of the affected muscles.
Stretching can be done in the
following ways:
- Self stretching, in which the
patient performs exercises at home (in Figure 5 it is explained it must be
applied on masseter and temporal), a)
- assisted stretching, in which the
therapist performs the muscular stretching manoeuvres
- stretching and spray, in which the
therapist combines to the elongation of the muscle, the surface spraying of the
contracted tract with ethyl chloride;
- stretching combined with
anaesthetic infiltration, in which the therapist stretches the muscle,
immediately after injecting local anaesthetic in the contracted tract. Page 109
………Furthermore after studies (Palla,
2001) it was shown that it is useful to subject the patient to any
physio-therapy treatment rather than leave him without assistance. b) Although
well-controlled clinical trials have not yet been published, it is recognized
as an effective and conservative treatment method. As already mentioned, it is
useful that the patient is trained to perform himself at home the treatment
modes, so that it becomes independent. This is also a great benefit from the
psychological point of view. Page 117
…………Stretching exercises are useful
for treating hardened and painful muscles and improve their relaxation (delayed
muscle pain, splinting, contracture, trigger points). b) They also increase the
radius of the movements of the joints. c)
To obtain muscle relaxation, a
proven result can be achieved by forcing the opening of the mouth against the
resistance given by the fist placed under the chin. In this case it is
exploited the principle of reciprocal innervation. To improve muscle strength
stabilization and isometric exercises are recommended, during them an action is
exerted against the fingers which push in an opposite direction........ d)
The coordination exercises are used
to achieve a coordinated and rhythmic muscle function. They are good in the
case of subluxation of an hypermobile TMJ. They are even effective on patients
who show deviations in the execution of movements due to muscle hyperactivity
………
Many patients do not do the exercises
if this increases the pain. In such cases, the physician must first obtain a
relief in symptoms through other means (plates, drugs or behavioural advice).
Once the patient has achieved a good result, the treatment plan should be
reassessed and modified over time to maintain optimal function. In any case we
do not recommend to provide the patient with a complicated exercise program
and/or a program requiring too much time to be executed, because there is the
risk that the patient gets tired and does not perform as specified. We think
that one or two exercises are the best choice. e)
These techniques are similar to
those used for muscle stretching and consist of forced movements of opening and
laterality of the jaw by both the therapist that self-administered by the
patient .....
Although such manoeuvres definitely
increase the radius of the mouth opening, it seems that a complete anatomical
reduction of the disc is not obtained (Okeson 1966). Obviously passive
movements must be performed by either the operator and the patient after TMJ
surgery, such as those carried out on other joints of the human body. f)
From the book by S. Palla
"Mioartropatie del sistema masticatorio e dolori orofacciali” RC Libri
2001
Physiotherapy treatment page 357
The physiotherapy is widely used in
the treatment of almost all rheumatic diseases. Physiotherapy measures are not
to be considered secondary or supporting therapies, but are an integral part of
the overall treatment plan. They are recommended by several Authors also as
therapy of myo-arthropathies, which are considered, as said, rheumatic
diseases. d)
1. Burgess JA, Sommers EE, Truelove
EL, et a/. Short-term effect of two therapeutic methods on myofascial pain and
dysfunction of the masticatory system. J Prosthet Dent 1988; 60:606-610.
2. Clark GT, Adachi NY, Dornan MR.
Physical medicine procedures affect tempomandibular disorder: a review. J Am
Dent Assoc 1990; 121: 151-162
3. Selby A. Physiotherapy in the
management of temporomandibular disorders. Aust Dent J 1985; 30: 273-280.
4. Sturdivant J, Fricton_JR.
Physical therapy for temporomandibular disorders and orofacial pain. Curr Opin
Dent 1991;1:485-496.
5. Zarb GA, Carlsson GE, Rugh JD.
Clinical management. In: Zarb GA. Carlsson GE, Sessle BJ, et al. (eds). Temporomandibular
joint and masticatory muscle disorders. Copenhagen Munksgaar d, 1994; 529-548.
Despite the lack of scientific
evidence about the therapeutic validity of physical therapy (see below), the
self-treatment of the patient with exercises and physiotherapy mode is deemed,
by our school, very important since the patient is involved from the outset in
the treatment and becomes co-responsible for his recovery. In addition, also
based on the results of a study (Feine JS, Lund JP. An assessment of the
efficacy of physical therapy and physical modalities for the control of chronic
muscoloskeletal pain. Pain 1997; 71: 5-23.), it is appropriate to subject the
patient to any physiotherapy treatment rather than leaving him with no
"attentions".
The aims of physiotherapy treatment
are:
1. pain control;
2. decrease in the tone and
lengthening of shortened masticatory muscles;
3. mobilization of hypomobile
joints. d)
These results are achieved with:
1.thermotherapy;
2.massage;
3.stretching exercises:
4.stabilization and coordination
exercises;
5. mobilization exercises.
Even stretching exercises are
intended to decrease the muscle tone and are particularly effective when the
musculature is previously contracted (post-isometric stretching. g)
Lewit K, Simons DG. Myofascial pain:
relief by post-isometric relaxation. Arch Phys Med Rehabil 1984; 65: 452-456.
There are three types of
techniques:
1. ballistic stretching;
2. static stretching;
3. contraction-relaxation stretching
or contraction-relaxation-contraction of the agonist muscle; the latter
technique is often called Proprioceptive Neuromuscular Facilitation (PNF) g)
Anderson B, Burke ER. Scientific, medical, and practical aspects of
stretching. Clin Sports Med 1991; 10: 63-86.
· Magnusson SP. Passive properties
of human skeletal muscle during stretch maneuvers. A review. Scand J Med Sci
Sports.
In the static stretching the muscle
is stretched as much as possible and hold in this position for 15/30 sec. The
PNF technique is based on the principle of reciprocal innervation: the muscle
is stretched and at the same time contracted for 6/8 sec. to 50 - 100% of the
maximum value. The contraction is followed by a new stretching phase.
Stretching exercises, i.e.
lengthening of the muscles, is a practice commonly used to treat hardened and
painful muscles, to improve sports performance, prevent muscle injuries, to
reduce muscle soreness after exercise and to increase the width of the
movement. d)
· Lewit K, Simons DG. Myofascial pain: relief
by post-isometric relaxation. Arch Phys Med Rehabil 1984; 65: 452-456.
· Magnusson SP. Passive properties
of human skeletal muscle during stretch maneuvers. A review. Scand J Med Sci
Sports 1998; 8: 65-67
Regardless of what mentioned above,
the evidence that stretching exercises are effective on pain is rather weak, at
least for the delayed or post-exercise muscle soreness.
It is found, however, that the
stretching exercises increase the amplitude of the movement c); this increase
was attributed to a decreased inhibition of muscular resistance to stretching,
to a change in the mechanical properties of muscle tissue and to a greater
tolerance of the patient to the stretching itself: the latter case seems to be
the most likely. The PNF technique is the one allowing greater muscle
elongation and, therefore, greater increase in the amplitude of the movement.
· Halbertsma JP, Goeken LN.
Stretching exercises: effect on passive extensibility and stiffness in short
hamstrings of healthy subjects (see comments). Arch Phys Med Rehabil
1994,75:976-981.
· Magnusson SP. Passive properties
of human skeletal muscle during stretch maneuvers. A review. Scand J Med Sci
Sports.
An extensive literature search,
conducted according to scientific standards, on the effectiveness of various
physiotherapy modes for the treatment of certain forms of musculoskeletal pain,
including those due to myo-arthropathy, came to the following conclusions:
• All treatments assessed have not
result in an improvement in symptoms of chronic musculoskeletal pain or quality
of patient's life able to outlast the period of treatment: the patient then
gets a short-term benefit from most of physiotherapy measures; h)
• talking about long-term, the
success of physiotherapy is not higher than that of a placebo treatment;
• by increasing the number of
treatment sessions more satisfactory results are obtained; i)
• patients derive greater benefit in
case they are subjected to any physiotherapy treatment than otherwise. J)
Feine JS, Lund JP. An assessment of
the efficacy of physical therapy and physical modalities for the control of
chronic muscoloskeletal pain. Pain 1997; 71: 5-23.
From these results it can be
inferred that all therapeutic modalities produce their beneficial effect
through a multiple action mechanism which reduces fear, depression and anxiety:
Malone MD, Strube MJ, Scogin FR.
Meta-analysis of non-medical treatments for chronic pain (published erratum
appears in Pain 1989 Apr;37(I):1281(see comments). Pain 1988; 34:23]1-244.
Patients may feel less pain,
engaging and focusing on other things, if fully informed and reassured about
their current situation and their future. k)
Feine JS, Lund JP. An assessment of
the efficacy of physical therapy and physical modalities for the control of
chronic muscoloskeletal pain. Pain 1997; 71: 5-23.)
It is known that, by diverting
attention away from the pain, the latter decreases in intensity. k) k)
· Bushnell MC, Duncan GH, Chen JI,
et al. Non-invasive brain imaging during experimental and clinical pain. In:
Devor M. Rowbotham MC, Wiesenfeld-Hallin Z (eds). Proceedings of the 9th world
congress on pain (Progress in pain research and management, Vol 16). Seattle:
IASP Press, 2000; 485-495
· Wall PD. Pain in context: the
intellectual roots of pain research and therapy. In: Devor M, Rowbotham MC,
Wiesenfeld-Hallin Z (eds). Proceedings of the 9th world congress on pain (Progress
in pain research and management, Vol 16). Seattle: IASP Press ,2000; 19-33
Chapter tile: "Stretching
exercises and mobilization" on page 396 (bibliography below)
Stretching and mobilization
exercises are indicated:
· as a therapy, in cases of mandibular
hypomobility;
· as prophylaxis of patients with
partially movable joint and also in patients having trouble in keeping the
mouth open or who can not open it sufficiently during dental therapy.
The patient is asked to open the
mouth fully, six times per day for six consecutive times, holding this position
for at least ten seconds (fig. 6 adn 7 page 397). For patients who have
difficulty in holding the mouth open, it can be effective to perform stretching
between by inserting between the incisors a series of overlapping wooden
paddles, many as they can be moved back and forth with the mouth fully open
(fig. 7). The exercise is performed properly when the paddles are not bitten.
If you want to reach a larger
opening of the mouth through a post-isometric stretching it is necessary:
· to bite the paddles for six
seconds with light pressure;
· relax muscles;
· when the relaxation occurred, open
the mouth to the maximum;
· as soon as possible introduce a
new paddle.
Repeat this exercise three or four times.
Bibliography:
1. Evjenth O, Hamberg J. Muscle
stretching in manual therapy. A clinical manual. Vol II. The spinal column and
the temporomandibular joint. Alfta: Alfta Rehab Forlag, 1984, 88-95.
2. Feldenkrais M. Awareness through
movement. New York: Harpers and Row, 1972.
3. Kaltenborn FM. Manuelle
Mobilisation der Extremitaten-gelenke. 9 ed. Oslo: Olaf Norlis Bokhandel, 1992;
114-179.
4. Maitland GD. Peripheral
manipulation. 3 ed. Oxford: Butterworth-Heinemann, I 991.
5. Maitland GD. Manipulation der
peripheren Gelenke. 2 ed. Berlin: Springer Verlag, 1996. 538-547
6. Capurso u, Marini I, Bonetti GA.
I disordini craniomandibolari. Fisioterapia speciale stomatognatica. Bologna:
Edizioni Martina, 1996.
7. Gerritsen GwJ. Physiotherapie bei
patienten mit Beschwerden des Kauapparates auf Grund einer myogenen
Fehlfunktion. In: Steenks MH, de Wijer A (eds). Kiefergelenkfunktionen aus
physiotherapeutischer und zahnmedizinischer Sicht. Diagnose und Therapie.
Berlin: Quintessenz, I99l; 133-142.
8. Hansson T, Honée W, Hesse J.
Funktionsstòrungen im Kausystem. Heidelberg: Dr. A. Hùthig Verlag, 1987.
9. Hansson TL, Christensen CA,
Taylor DLW. Physical therapy in craniomandibular disorders. Chicago:
Quintessence, 1992.
10. Klein-Vogelbach S. Therapeutische
Ubungen zur funktionellen Bewegungslehre. 3 ed. Berlin: Springer Verlag, 1993;
164-167.
11. Kraus S.L. TMJ disorders.
Management of the craniomandibular complex. NewYork: Churcill Livingstone,
1988; 139-173.
12. Langedoen-Sertel J. Die
Bedeutung des retrodiskalen Gewebe bei temporo-mandibulàren Arthropathien.
Manuelle Therapy 1998;2: 8-4.
13. Langedoen J, Múller J, Jull GA.
Retrodiscal tissue of the temporomandibular joint: clinical anatomy and its
role in the diagnosis and treatment of arthropathies. Manual therapy 1997; 2:
191-198
14. Langendoen- Sertel J.
Physiotherapie und MRT Funktionsdiagnostik einer intraartikulàren
Kiefergelenksdyfunktion. Manuelle Medizin 1997; 6: 319-321.
15. McKenzie RA. The cervical and
thoracic spine. Mechanical diagnosis and therapy. Waikanae (NZ): Spinal
publications, 1992.
16. McKenzie RA. Treat your own
neck. 3 ed.Waikanae (NZ): Spinal Publications, 1996.
17. Simons DG, Travell JG, Simons
LS. Myofascial pain and dysfunction. The trigger point manual. Volume 1. Upper
half of body. 2 ed. Baltimore: Williams & Williams, 1999; 237 -415 .
Considerations regarding the manual
stretching technique
a) All authors recommending the
stretching do meant it limited to the practice in the dental office, but
recommend it also at the patient's home, so that he is trained to become
independent in pain control. This is also a great benefit from the
psychological point of view. It is therefore an harmless practice, in all the
bibliography cited above any case of unfavourable, neither serious nor mild
event is cited.
b) Although not playing a
fundamental role in pain therapy it is a valuable therapeutic aid when
integrated in the dental treatment of temporomandibular joint pain.
c) It increases considerably the
radius of the movements of the joints (stretching) increasing the opening of
the mouth. It controls the pain. This is an undoubted benefit because it allows
the dentist to work more efficiently in any situation (conservative,
endodontics, surgery, implants, etc.). At the same time it reduces the fatigue
of the patient and the risk that holding the mouth open for a long time could
induce the appearance or worsening of muscle pain. In the case of dental
extractions consider that in addition to being a long time with his mouth open,
also a strong asymmetric force is exerted in the patient's mouth, and all
result in the onset of pain in the muscles of the masticatory system. The
indication for guided implantology requires a larger opening of the oral
cavity, to be maintained for a long time.
d) The exercises currently described
take place forcing the mouth against an opposing resistance given by the fist
placed under the chin, or stabilization and isometric exercises are
recommended, during them an action is exerted against the fingers that push in
the opposite direction . The use of a simple compressed spring facilitates the
execution of stretching acting in the same manner, contraction opposite to
force. Physiotherapy is widely used in the treatment of most rheumatic diseases,
including myo-arthropathies. Physiotherapy measures are an integral part of the
overall treatment plan. In the presence of contraction of the muscles of the
temporomandibular joint system and detection of the relationship between the
dental arches (bite mio-centric, skull mandibular relationship, etc.) allows
the possibility to relax the muscles. This allows a better assessment of the
masticatory system (including the possibility of increasing the spaces between
the arches) and an easier detection of the intermaxillary relationship,
regardless of the technique chosen. Relax muscles and increase the opening of
the mouth allow to apply with greater ease the technique chosen, classical
gnathology, Planas technique, Alonso, Jankelson, etc..
e) The scientific literature does
not recommended to provide the patient with an exercise program complicated
and/or requiring too much time to be performed, because there is the risk that
the patient gets tired and does not perform as specified. One or two exercise
are referred to as the optimal choice. The course of physiotherapy with the
"oral dynamic stretching" allows to simplify the execution of
physiotherapy exercises.
f) It useful in surgery of the
temporomandibular joint.
g) The stretching movements are
particularly effective when the muscle is previously contracted (post-isometric
stretching). Contraction-relaxation stretching or
contraction-relaxation-contraction of the agonist muscle called Proprioceptive
Neuromuscular Facilitation (PNF) is more effective than other types of
stretching (e.g. static). The muscle is stretched and, at the same time, is
contracted for 6/8 sec. to 50 - 100% of the maximum value. The contraction is
followed by a new stretching phase. This method is easily applicable with the
device called "dynamic oral stretching."
h) All therapies assessed have
result in an improvement in symptoms of chronic musculoskeletal pain or quality
of patient's life for the duration of the treatment period: the patient, then,
gets a benefit by most physiotherapy measures; i)
i) increasing the number of therapy
sessions more satisfactory results are obtained;
j) patients derive greater benefit
if subject to any physiotherapy treatment than otherwise.
k) All therapeutic modalities
produce their beneficial effect through a multiple action mechanism which
reduces fear, depression and anxiety By diverting attention away from the pain,
the latter decreases in intensity. Having to use a stretching spring
"distracts" the patient, helping to reduce the intensity of pain.
The "TheraBite" a similar
device with the same indications
The web-site
http://www.atosmedical.com/Corporate/Focus_areas/Mouth_and_Jaw/The_TheraBite_System.aspx
says:
The TheraBite ® Jaw Motion
Rehabilitation System™ is a portable system specifically designed to treat
Trismus and mandibular hypomobility. The system uses a repetitive passive
motion and stretching for an effective jaw rehabilitation therapy useful to:
Restore the mobility and flexibility
of the muscles of the jaw, joints, and connective tissues, thereby increasing
the opening of the jaw, this mobilization is crucial in reducing inflammation
and pain. The mouth opening may be limited by internal factors, for example,
bony ankylosis, arthritis, infection, trauma; a scar in the fibrous tissue can
cause stiffening of joints and muscles and requires stretching for
re-lengthening the collagen fibres. Probably also a micro-trauma may involve
bruxism..
· It relieves muscle pain
(myofascial), usually caused by abnormal inflammation that exerts pressure on
nerves, muscles and bones. This inflammatory process can be corrected througha
range of passive movement exercises.
· Mandibular Trismus; is a
debilitating condition that can affect people of all ages. If not properly and
promptly treated, the condition can worsen and have a negative impact on
quality of life.
· After surgery and maxillary
radiation; the joints that have been immobilized may undergo degenerative changes
within a few days.
· Disorders of the temporomandibular
joint (TMJ);
· TMJ trauma.
· helps to increase mass and
strength in hypotonic muscles;
·reduce anxiety in patients,
allowing them to control muscle function.
· strengthen the weakened muscles of
the jaw.
Within the site the mechanisms that
lead to trismus are deepened and several related physiopathogenetic mechanism
are discussed.
The trismus can result from muscle,
articular damage, rapid growth of connective tissue (scars), or a combination
of these factors.
alterations of the central nervous
system, trigeminal injury, drug and medication toxicity may also limit the
opening of the mouth.
The mandibular trismus may occur as
a result of:
· Third molar extraction
· hyperextension
· hematoma resulting from injection
of the dentist,
· as delayed effect of fixation
after mandibular fracture or other trauma.
· Radiation therapy to the head and
neck.
· Surgery of the head and neck
· TMJ Disorders
· Infections
· Systemic diseases, such as
rheumatoid arthritis or scleroderma
· direct trauma to the head and
neck;
· Indirect trauma, for example,
whiplash
· Burns of the face
· Stress due to disorders, for
example, bruxism.
· Congenital (at birth)
· because of hereditary diseases
· because of ageing
Regardless of the immediate cause,
Trismus (mandibular hypomobility) will ultimately result in degeneration of the
muscles and joints. Studies have shown that muscles that are not able to pass
through their range of motion for no longer than 3 days begins to show signs of
atrophy.
Similarly, the joints that are
immobilized quickly begin to show degenerative changes, such as thickening of
the synovial fluid and the thinning of the cartilage.
When patients receive radiation
treatment in the head and neck, Trismus may also progress slowly and unnoticed
for months, causing minor changes in muscles and joints.
Therefore, the treatment, consisting
in a gentle passive movement, should begin as soon as possible.
In the Instruction Manual attached
the following indications are described:
The TheraBite system helps to
achieve:
1.Correct opening of the jaw: by
stretching the connective tissue mobilizing the joints stretching the muscles
completely.
2.Relieve of pain and inflammation.
3.passive mobilization of join.
Researches have highlighted the beneficial effects of mobilization in the
management of joint disorders. The movement is necessary to prevent the
degeneration of the cartilage, the tissue layer that covers most of the
articular surfaces.
4. In many cases it can stimulate
healing of the joint and reduce pain and swelling.
5. Stretching and relaxing muscles,
gradual mobilization exercises can help patients suffering from muscle pain to
improve movement.
6.Passive movement may also offer
therapeutic advantages, especially in the post-operative period.
This rehabilitation exercise of the
jaw is effective when carried out every day. It allows to be used wherever the
patient is.
The TheraBite system has been used
successfully by thousands of individuals suffering from Trismus.
In countries like the United States
(Medicare) and Germany, the TheraBite system is approved for reimbursement by
the insurance company. This rule varies from state to state and from country to
country.
A disposable scale used to measure
the range of motion in scale allows patients and their doctors to measure the
exact mandibular opening, monitoring progress.
A graph allows to assess the
measurement of the patient's progress and allows users and their doctors to
monitor progress through a visual feedback ....
The aid assists the patient to
maintain constant the static opening and the force applied during stretching.
It is preferable that the therapy
with TheraBite is monitored by health care professionals.
REFERENCES
1. Buchbinder D, Currivan RB, Kaplan
AJ, Urken ML. Mobilization regimens for the prevention
of jaw hypomobility in the radiated
patients. A comparison of three techniques. Journal of Oralmaxillofacial
Surgery. 1993; 512363467.
2. Maloney GE, Mehta N, Forgione AG,
Zazawi KH, Al-Badawi EA, Driscoll SE. Effects of a
passive jaw motion device on pain
and range of motion in TMD patients not responding to flat plane intraoral
appliances. The Journal of CranioMandibular Practice, 2002; 20:55-66.
3. Messing BP, Saunders JR,
Dietrich-Burns K, Farrell SS, Pyrke-Fairchild J, Melick CF. Trismus
management in the head and neck
cancer patient undergoing organ preservation treatment. 6th International
Conference on Head and Neck Cancer, Washington DC, USA August 07-11, 2004.
Scientific Poster 01-97.
4. Bandy WD, Irion JM, Briggler M.
The effect of static stretch on the flexibility of the hamstring muscles.
Physical Therapy 1997; 77: 1090-1096.
a. Cohen GS, Fletcher M. Comparison
of Jaw Mobilization Regimens. Journal of Dental Research, 1991; 70:329.
5. Clark HM. Neuromuscular
Treatments for Speech and Swallowing: A Tutorial. American Journal of
Speech-Language Pathology. 2003; 12:400-415.
6. De Deyne PG. Application of
passive stretch and its implications for muscle fibers. Physical Therapy. 2001;
812321422.
7. Frank C, Akeson WH, Woo SL-Y,
Amiel D, Ing D, Coutts RD. Physiology and therapeutic value of passive joint
motion. Clinical Orthopaedics and Related Research 1984; 185:113-120.
8.Gassner R, Buckley M, Studer RK,
Evans CH, Agarwal S. Interaction of strain and interleukinin articular
cartilage: effects on proteoglycan synthesis in chondrocytes; International
Journal of Oral and Maxillofacial Surgery 2000; 29:389-394.
9. Gaziano JE. Evaluation and
management of oropharyngeal dysphagia in head and neck cancer. Cancer Control.
2002; 9: 400-408.
10. Milam S, Zardeneta G. Oxidative
stress and degenerative temporomandibular joint disease
A proposed hypothesis. Journal of
Oral and Maxillofacial Surgery 1998; 56:214-223.
11. Nicolakis P, Burak E, Kopf A,
Djaber-Ansari A, Piehslinger E, Fialka-Moser V, Exercise therapy for
craniomandibular disorders: Archives of Physical Medical Rehabilitation, 2001;
81:1137-1141.
12. Nicolakis P, Burak EC, Kollmitzer
J, Kopf A, Piehslinger E, Wiesinger GF, Fialka-Moser V. An investigation of the
effectiveness of exercise and manual therapy in treating symptoms of TMJ
osteoarthritis. Cranium: The Journal of Crianiomandibular Practice. 2001;
19(1):26-32
13. Nicolakis P; Erdogmus B; Kopf A;
Nicolakis M; Piehslinger E; Fialka-Moser V
Effectiveness of exercise therapy in
patients with myofascial pain dysfunction syndrome. Journal of Oral
Rehabilitation. 2002; 29(4):362-368.
14.Salter RB The biological concept
of continuous passive motion of synovial joints; the first 18 years of basic
research and its clinical application. Clinical Orthopaedics and Related
Research: 1989:242: 12-26.
15.Sapega AA, Quedenfeld TC, Moyer
RA, Butler RA. Biophysical factors in range-of-motion exercise. Physical Sports
Medicine. 1981; 9(12):57-61.
Bruxism and stretching
Knutson GA Vectored
upper cervical manipulation for chronic sleep bruxism, headache, and cervical
spine pain in a child. J Manipulative Physiol Ther. 2003 Jul-Aug;26(6):E16.
1.De Laat A, Stappaerts K, Papy S. Counseling and
physical therapy as treatment for myofascial pain of the masticatory
system. J Orofac Pain. 2003
Winter;17(1):42-9.
2.Visscher CM, Lobbezoo F, Naeije M. [Treatment of
bruxism: physiotherapeutic approach] [Article in Dutch] Ned Tijdschr Tandheelkd.2000
Jul;107(7):293-6.
3.Quinn JH. Mandibular exercises to
control bruxism and deviation problems. Skull 1995 Jan;13(1):30-4.
Stretching increases the range of
motion
1.Magnusson SP. Passive properties
of human skeletal muscle during stretch maneuvers. A review. Scand J Med Sci
Sports 1998; 8: 65-67
2.Halbertsma JP, Goeken LN.
Stretching exercises: effect on passive extensibility and stiffness in short
hamstrings of healthy subjects (see comments). Arch Phys Med Rehabil
1994,75:976-981.
3.Magnusson SP. Passive properties
of human skeletal muscle during stretch maneuvers. A review. Scand J Med Sci
Sports. 1998 Apr;8(2):65-77.
4.Lewit K, Simons DG. Myofascial
pain: relief by post-isometric relaxation. Arch Phys Med Rehabil 1984; 65:
452-456.
Stretching increases the flexibility
of skeletal muscles.
1.C. Holzman Weppler, S. P.
Magnusson Increasing Muscle Extensibility: A Matter of Increasing Length or
Modifying Sensation? Physical Therapy March 2010 vol. 90 no. 3 438-449
2.S P Magnusson, E B Simonsen, P
Dyhre-Poulsen, P Aagaard, T Mohr and M Kjaer. Phys Ther in press in
press Viscoelastic stress relaxation during static stretch in human
skeletal muscle in the absence of EMG activity.
3.O Aura and P V Komi Effects
of prestretch intensity on mechanical efficiency of positive work and on
elastic behavior of skeletal muscle in stretch-shortening cycle exercise. Phys Ther in press.
4.Ulrike H Mitchell, J William
Myrer, J Ty Hopkins, Iain Hunter, J Brent Feland and Sterling C Hilton. Acute
stretch perception alteration contributes to the success of the PNF
"contract-relax" stretch. Phys Ther in press
5. Exercise
adherence in patients with trismus due to head and neck oncology: a qualitative
study into the use of the Therabite.
6. Melchers LJ, Van Weert E,
Beurskens CH, Reintsema H, Slagter AP, Roodenburg JL, Dijkstra PU.
7.Int J Oral Maxillofac Surg. 2009
Sep;38(9):947-54. Epub 2009 May 2.
8.Treatment
of bilateral hyperplasia of the coronoid process of the mandible. Presentation
of a case and review of the literature.
9.Fernández Ferro M, Fernández
Sanromán J, Sandoval Gutierrez J, Costas López A, López de Sánchez A, Etayo
Pérez A.
10.Med Oral Patol Oral Cir Bucal.
2008 Sep 1;13(9):E595-8. Review.
11.The
effect of cervical spine manual therapy on normal mouth opening in asymptomatic
subjects.
12.George JW, Fennema J, Maddox A,
Nessler M, Skaggs CD.
13.J
Chiropr Med. 2007 Dec;6(4):141-5.
14.Fourteen-year follow-up of a
patient-fitted total temporomandibular joint reconstruction system.
15.Mercuri
LG, Edibam NR, Giobbie-Hurder A.
16.
J Oral Maxillofac Surg. 2007 Jun;65(6):1140-8.
17.Use of a Therabite appliance in the
management of bilateral mandibular coronoid hyperplasia.
18.Gibbons
AJ, Abulhoul S.
19.Br
J Oral Maxillofac Surg. 2007 Sep;45(6):505-6. Epub 2006 Jul 13.
20.Early
use of a mechanical stretching device to improve mandibular mobility after
composite resection: a pilot study.
21.Cohen EG, Deschler DG, Walsh K,
Hayden RE.
22.Arch Phys Med Rehabil. 2005
Jul;86(7):1416-9.
23. Preemptive
rofecoxib and dexamethasone for prevention of pain and trismus following third
molar surgery *.
24.Moore PA, Brar P, Smiga ER,
Costello BJ.
25.Oral Surg Oral Med Oral Pathol
Oral Radiol Endod. 2005 Feb;99(2):E1-7.
26.Trismus
in head and neck oncology: a systematic review.
27.Dijkstra PU, Kalk WW, Roodenburg
JL.
28.Oral Oncol. 2004
Oct;40(9):879-89. Review.
29.Long-term
follow-up of the CAD/CAM patient fitted total temporomandibular joint
reconstruction system.
30.Mercuri LG, Wolford LM, Sanders
B, White RD, Giobbie-Hurder A.
31.J Oral Maxillofac Surg. 2002
Dec;60(12):1440-8.
32.Horst,
CEO of Therabite Corp., comments on Stiesch-Sholtz article in April 2002
CRANIO.
33.Horst R.
34.Cranio. 2002 Jul;20(3):151. No
abstract available.
35.Effect
of a passive jaw motion device on pain and range of motion in TMD patients not
responding to flat plane intraoral appliances.
36.Maloney GE, Mehta N, Forgione AG,
Zawawi KH, Al-Badawi EA, Driscoll SE.
37.Cranio. 2002 Jan;20(1):55-66.
38.The
Christensen prosthesis. A retrospective clinical study.
39.Chase DC, Hudson JW, Gerard DA,
Russell R, Chambers K, Curry JR, Latta JE, Christensen RW.
40.Oral Surg Oral Med Oral Pathol
Oral Radiol Endod. 1995 Sep;80(3):273-8.
41.Mobilization
regimens for the prevention of jaw hypomobility in the radiated patient: a
comparison of three techniques.
42.Buchbinder D, Currivan RB, Kaplan
AJ, Urken ML.43.J Oral Maxillofac Surg.
1993 Aug;51(8):863-7






.jpg)


{kind=link}
{kind=link}
{kind=link}
{kind=link}